Differentiating atrioventricular (AV) blocks is a simple process as long as you understand some of the patterns. Here I will explain the different AV blocks, describe the part of the AV nodes involved in each block, and then show you how to figure one out from the other. These are all explained further and with visual examples in my video course, Executive Electrocardiogram Education (ecgedu.com).
What Are The Different Atrioventricular (AV) Blocks
ECG readers define four basic atrioventricular (AV) blocks. Some are overall benign, but some are dangerous. The AV blocks include first-degree AV block, second-degree AV block, third-degree (complete) AV block, and 2:1 AV block. Second-degree AV block further divides into two categories – second-degree AV block, Mobitz type 1 (Wenckebach), and second-degree AV block, Mobitz type 2. I describe each of these blocks below.
Understanding the Atrioventricular (AV) Node
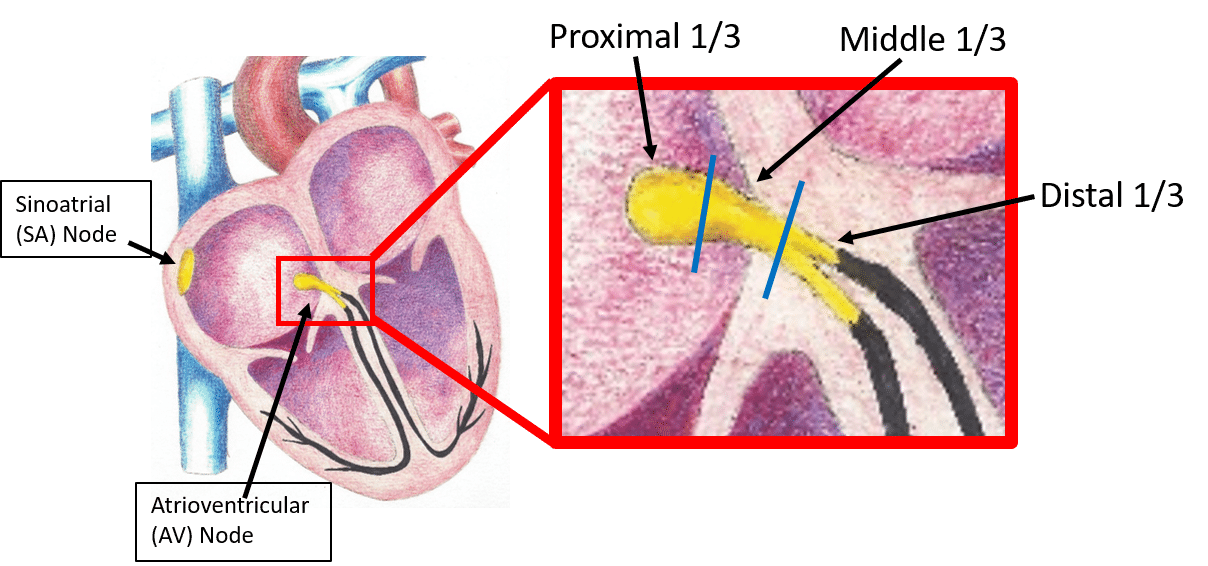
The atrioventricular node is a small area of conduction located at the top of the ventricular septum, between the atria and the ventricles. Although distinct tracts are not truly there, it is easier to think of the AV node as a series of wires. Additionally, the AV node can be mentally divided into three sections – the proximal third, the middle third, and the distal third.
“Wiring” of the Atrioventricular (AV) Node
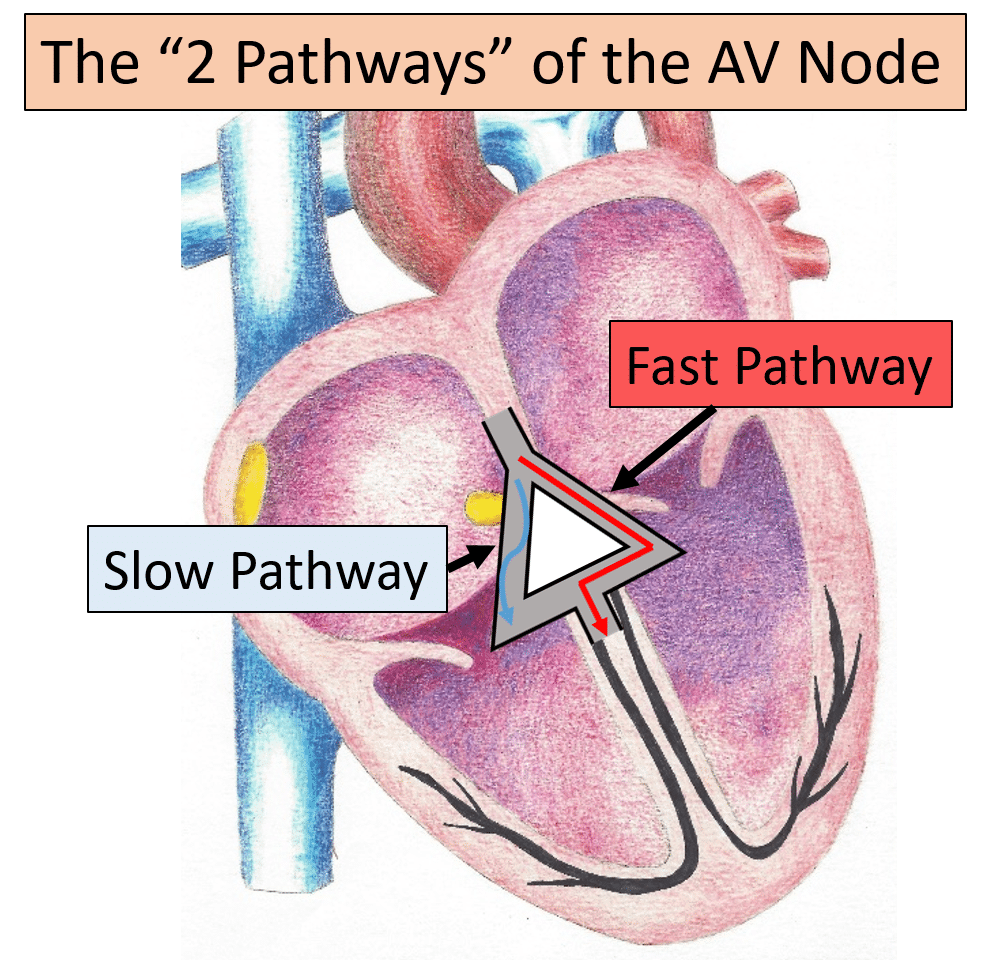
The atrioventricular node consists of two pathways. The fast pathway, depicted on the right of the picture, and the slow pathway, depicted on the left of the picture. These two pathways play a role in AV nodal tachyarrhythmias such as atrioventricular nodal reentrant tachycardia (AVNRT). Since this article describes AV blocks, I will not go into further detail about these pathways at this time.
“Divisions” of the Atrioventricular (AV) Node
Proximal Third of the AV Node
For practical purposes, the AV node divides into three sections. When the proximal third is affected, there is a slowing of conduction from the atria into the ventricle. This is the area responsible for first-degree atrioventricular blocks and second-degree AV blocks, Mobitz type 1 (Wenckebach). Abnormalities within the proximal third of the AV node are typically benign and do not degenerate into more malignant blocks or abnormalities.
Mid and Distal Third of the AV Node
The second and third parts of the AV node extend into the bundles of the left ventricles and abnormalities in these areas are significant. Abnormalities within these areas are responsible for second-degree atrioventricular blocks, Mobitz type 2 and third-degree (complete) AV blocks. Patients with these conduction delays often require a pacemaker.
The Different Atrioventricular (AV) Blocks in Detail
First-Degree AV Block
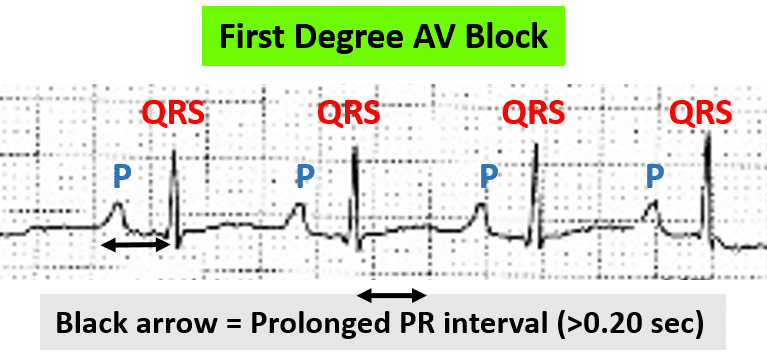
First-degree AV block occurs due to slowing of the first third of the atrioventricular node. This delay manifests on the electrocardiogram (ECG) as a prolongation of the PR interval (the beginning of the P wave to the beginning of the QRS complex). Normally the PR interval is 0.12 to 0.20 seconds. With the first-degree AV block, the PR interval is >0.20 seconds.
Second-Degree AV Block, Mobitz Type 1 (Wenckebach)
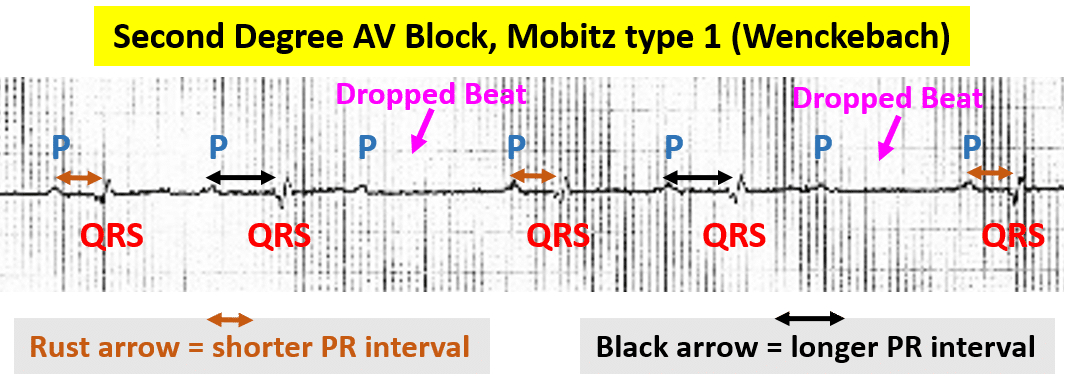
Second-degree AV block, Mobitz type 1 (Wenckebach) occurs due to progressive fatiguing of the first third of the AV node. During these cycles, the first atrial impulse conducts through the AV node. The next impulse also conducts through the AV node, but a little slower. The next impulse conducts even slower. This continues until the AV node fatigues and no longer conducts a beat to the ventricles. There is now a “dropped beat,” (no QRS complex after the P wave).
The ECG shows a P wave, a relatively short PR interval, and a QRS complex, followed by another P wave, a longer PR interval, and a QRS complex, followed by another P wave, and no QRS complex.
Second-Degree AV Block, Mobitz Type 2
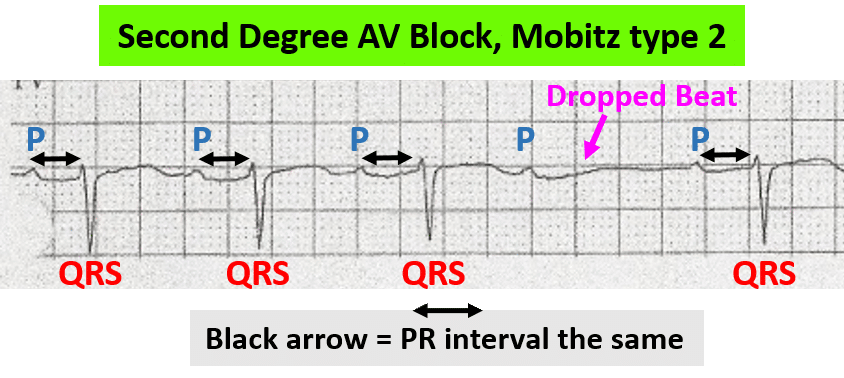
Second-degree AV block, Mobitz type 2 occurs due to significant disease of the second and/or third sections of the AV node. With this AV block, conduction goes down the AV node relatively normally at times and then ceases at times. A classic pattern shows a P wave and a QRS complex, followed by another P wave and QRS complex with the same PR interval, followed by additional P waves and QRS complexes with the same PR interval, and then a P wave with no QRS complex following.
This image shows this. You see P wave, QRS, then P wave, QRS, then P wave, QRS, and finally a P wave and no QRS. Due to a diseased AV node, conduction through the node may just stop.
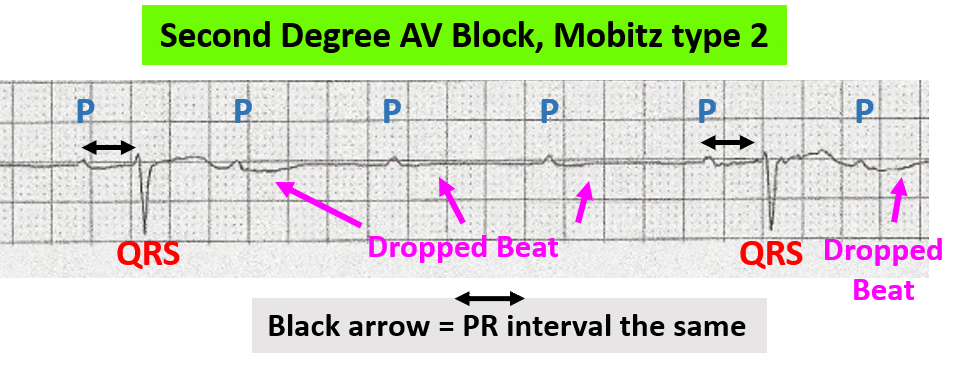
Another pattern of second-degree AV block, Mobitz type 2 may be multiple P waves that do not conduct impulses to the ventricles and then occasional atrial impulses (P waves) that do conduct and produce ventricular beats (QRS complexes). You see this in this rhythm strip. There is a P wave, no QRS, a P wave, no QRS, a P wave, no QRS, and finally a P wave followed by a QRS. This pattern continues.
Third-Degree (Complete) AV Block
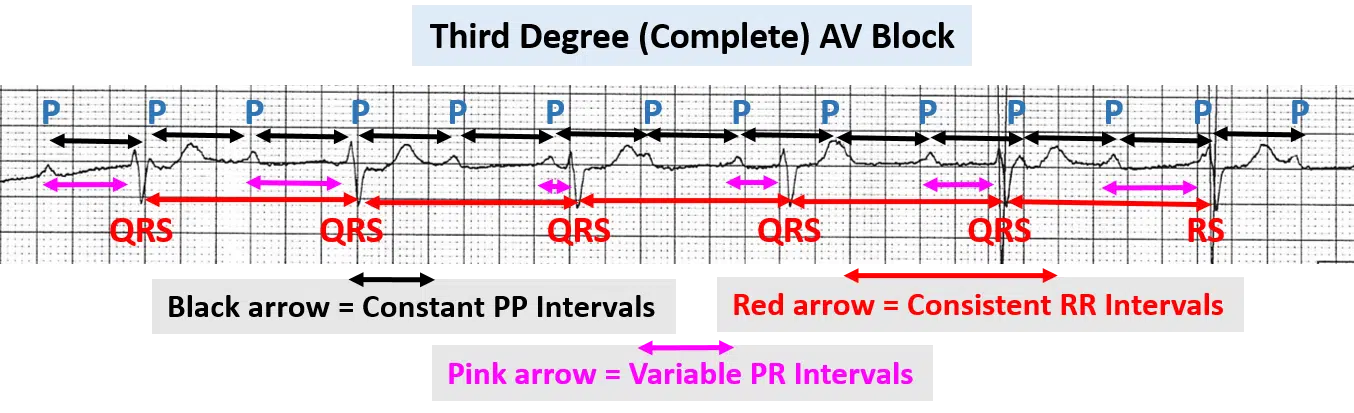
Third-degree (complete) atrioventricular blocks occur due to severe disease of the second or third portions of the AV node. Here there is no conduction from the atria to the ventricles. As such, the atria produce their own rhythm and ventricular tissue is forced to rely on its intrinsic pacemaker properties to produce its own rhythm. Essentially, you see an atrial rhythm with regularly timed P waves superimposed on a rhythm strip with regularly timed and slower QRS complexes. The PR intervals all vary since neither rhythm interacts with the other.
This image of third-degree AV block shows regularly spaced P waves (black arrows) and regularly spaced QRS complexes (red arrows) together. You can see variations in the PR intervals (pink arrows).
2:1 AV Block
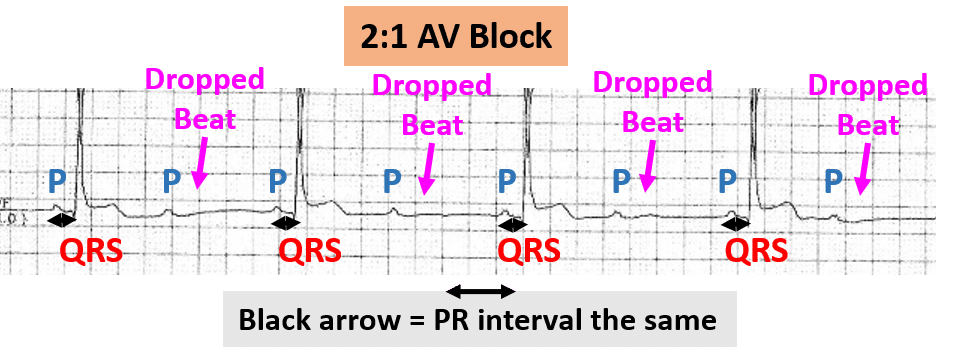
2:1 AV block is simply a repeating pattern of a P wave followed by a QRS complex, followed by a P wave, and no QRS complex. As the name implies, there are two P waves for every one QRS complex. This pattern can represent either second-degree AV block, Mobitz type 1, or Mobitz type 2, but there is not long enough to see if there is PR interval variation. Since this AV block can be either type 1 or type 2, any part of the AV node may be affected.
In this example of the 2:1 AV block, you see P wave, QRS, P wave, dropped beat. The pattern repeats.
Summary of Atrioventricular (AV) Blocks
Atrioventricular blocks can be summarized in a brief table like the one below. One looks at the PP intervals, the PR intervals, The RR intervals.
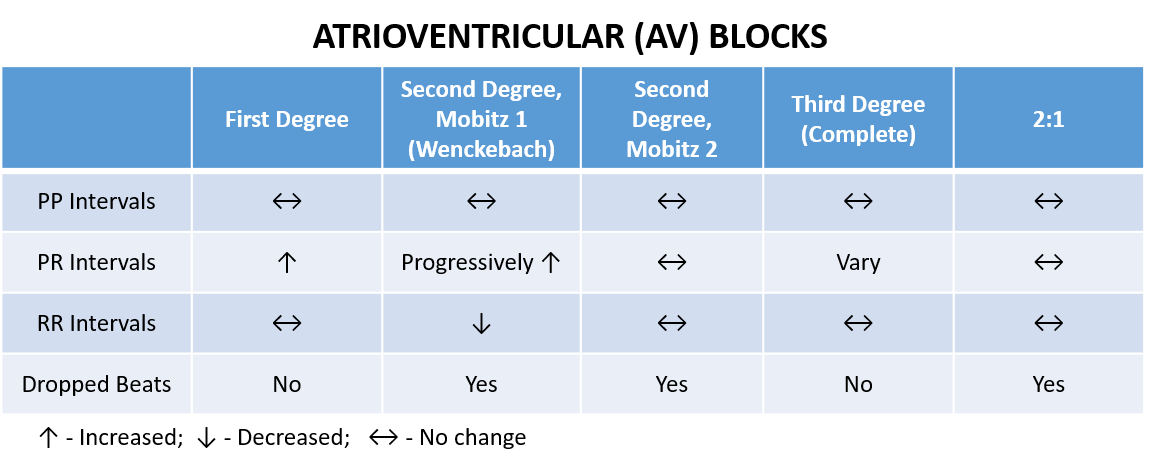
PP Intervals
The PP interval is always constant because this is not a problem with the sinus node. The sinus node continues to give off beats in regular intervals regardless of the AV block.
PR Intervals
With first-degree AV block, the PR intervals are all constant, but prolonged. With second-degree AV block, Mobitz type 1 (Wenckebach), the PR intervals progressively increase before the dropped beat. With second-degree AV block, Mobitz type 2, the PR intervals remain the same before the dropped beat.
RR Intervals
Although difficult to see, with second-degree AV block, Mobitz type 1, the RR intervals shorten from beat to beat before the dropped beat. With second-degree AV block, Mobitz type 2, the RR intervals remain the same before the dropped beat.
Third-Degree AV Block Intervals
With third-degree AV block, the PP intervals stay the same, the RR intervals stay the same and the PR intervals vary.
Conclusion
Understanding atrioventricular blocks is actually simple and logical. All you need is a little knowledge and you will be able to recognize the patterns in no time.
Learn about atrioventricular (AV) blocks, plus much more with Executive Electrocardiogram Education (ecgedu.com), an all-inclusive, online video course. You will learn all of the ECG and arrhythmia basics, such as lead placement, atrial and ventricular arrhythmias, myocardial ischemia, injury, and infarction, plus much more. Additionally, you will learn an approach to reading ECGs and arrhythmias that is not offered in other courses. Check out the sample videos and at the very least sign up for the free advanced cardiac life support (ACLS) video tutorial and quiz.

